I have written several times on syndactyly, most recently about an unusual case of thumb- index syndactyly http://congenitalhand.wustl.edu/2013/08/thumb-index-syndactyly.html
I have also mentioned (but not discussed in great detail) partial syndactyly. Partial syndactyly means that the fingers are joined together by a skin bridge without bony connection. The skin bridge does NOT travel all the way to the fingertip (thus, partial). Many times the skin bridge is short, only to the first knuckle (the PIP joint). Partial syndactyly may or may not cause functional problems. Often the partial syndactyly involves the long finger and the ring finger (also most common site for complete syndactyly– which is a joining of the skin to the fingertip). Syndactyly between the long and ring finger can limit spread of the fingers and limits the ability to wear a ring (perhaps a wedding ring, one day). Partial syndactyly of the index and long finger can tether the index finger and affect pinch activities- patients/ families do complain about this aspect. And, as always, there is the appearance issue which really does matter to patients and to families.
When I meet a patient/ family with a partial syndactyly, we discuss the nature of the syndactyly and I learn how it affects the child. For some, the partial syndactyly is simply not a big deal and no intervention is recommended. For others, the syndactyly limits function. In those patients with functional limitations, surgery is discussed. Surgery in those patients who simply want the syndactyly treated for appearance reasons is rare but does happen (in my mind, this discussion includes those who want to be able to wear a ring). I frankly discuss the difficulties of surgery, the healing process, the risks, etc. Some will chose surgery.
Surgical protocol.
Surgery is outpatient meaning you can go home that night. I use a big, bulky but soft dressing for most patients but occasionally for the younger child will use an above elbow cast. I typically leave the dressing on for about 3 weeks. I use dissolving sutures so nothing to remove. Depending on the appearance of the wound, sometimes we use a dry dressing and sometime we use an odoform support at night (and splint at night). Scar massage is instituted when the sutures start to dissolve.
 |
| Partial syndactyly between the index and long fingers. Not severe but functionally limiting. |
 |
| Partial syndactyly view from palm |
 |
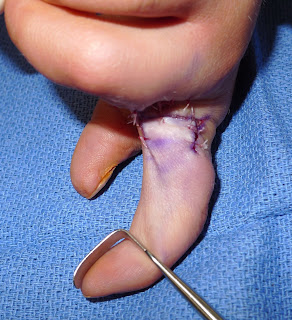
| After syndactyly reconstruction with dorsal commissural flap. |
Another case demonstrating the box flap technique. This 3 flap technique is effective in covering the partial syndactyly is some patients.
 |
| Box flap design for recurrent syndactyly reconstruction. |
 |
| Corrected syndactyly with box flap |
 |
| Box flap reconstruction with flaps in place. |
Partial syndactyly of the long and ring fingers. The first case is corrected by a dorsal first metacarpal artery flap. See the diagram of the flap.
 |
| Partial syndactyly between long and ring fingers |
 |
| Partial syndactyly flap reconstruction (without skin grafts) |
Other long and ring finger partial syndactyly.
 |
| Partial syndactyly past the PIP joint. This is a longer than typical partial syndactyly. |
 |
| Partial syndactyly from palm |
 |
| Additional syndactyly |
 |
| Additional partial syndactyly |











