Phocomelia is Greek for ‘seal limb’, a descriptive term for a short, deficient arm (or leg). I have previously posted on this topic HERE. For many years, patients with a really short arm were diagnosed with phocomelia as it became a ‘wastebasket’ term for such patients. However, the term should be used in patients with an intercalary deficiency, that is, a deficiency primarily of one segment of the extremity (and NOT, for a generally short limb). For example, a phocomelia could be a patient with a near normal humerus bone and a near normal hand without a forearm. Or a near normal forearm and hand without a humerus. Such patients are extremely rare today but the term and appearance became common nearly 60 years ago related to use of thalidomide by pregnant women.
So, back to our focus- the really short arm and deficient hand. Most commonly, this is NOT phocomelia but more likely is severe
radial or ulnar deficiency. We first identified and reported this connection in the medical literature in 2005, summarized
HERE. Recently, I met a new adult patient with an undiagnosed left arm deficiency. We had a long discussion about any diagnosis as well as her concerns that this may relate to her father’s exposure to Agent Orange in Vietnam. There is no evidence that I can find relating to any parental exposure. But, her clinical appearance and the x-rays suggest a diagnosis of
ulnar longitudinal deficiency. I have written a good deal about
ulnar longitudinal deficiency previously, found
HERE. There is also good additional information to be found on
Orphanet,
OMIM including ulnar mammary syndrome (
UMS), and others.
To me, making the correct diagnosis is important for many reasons. One reason is simple- peace of mind. Giving a name and diagnosis to a condition helps decrease anxiety around a condition. It also provides information to the family. Also, the correct diagnosis gives genetic information which may be important for future generations. Finally, the right diagnosis helps identify other associated abnormalities of the skeleton or the key organs (like heart, lungs, etc). In ulnar longitudinal deficiency, the main associated anomaly is trouble at the lateral ankle (distal fibula) and, very rarely, a severe deficiency of the hip. There are not other regular conditions of the bones or key organs. This is different than other similar conditions, like radial longitudinal deficiency, with known heart, spine, kidney, and other conditions.
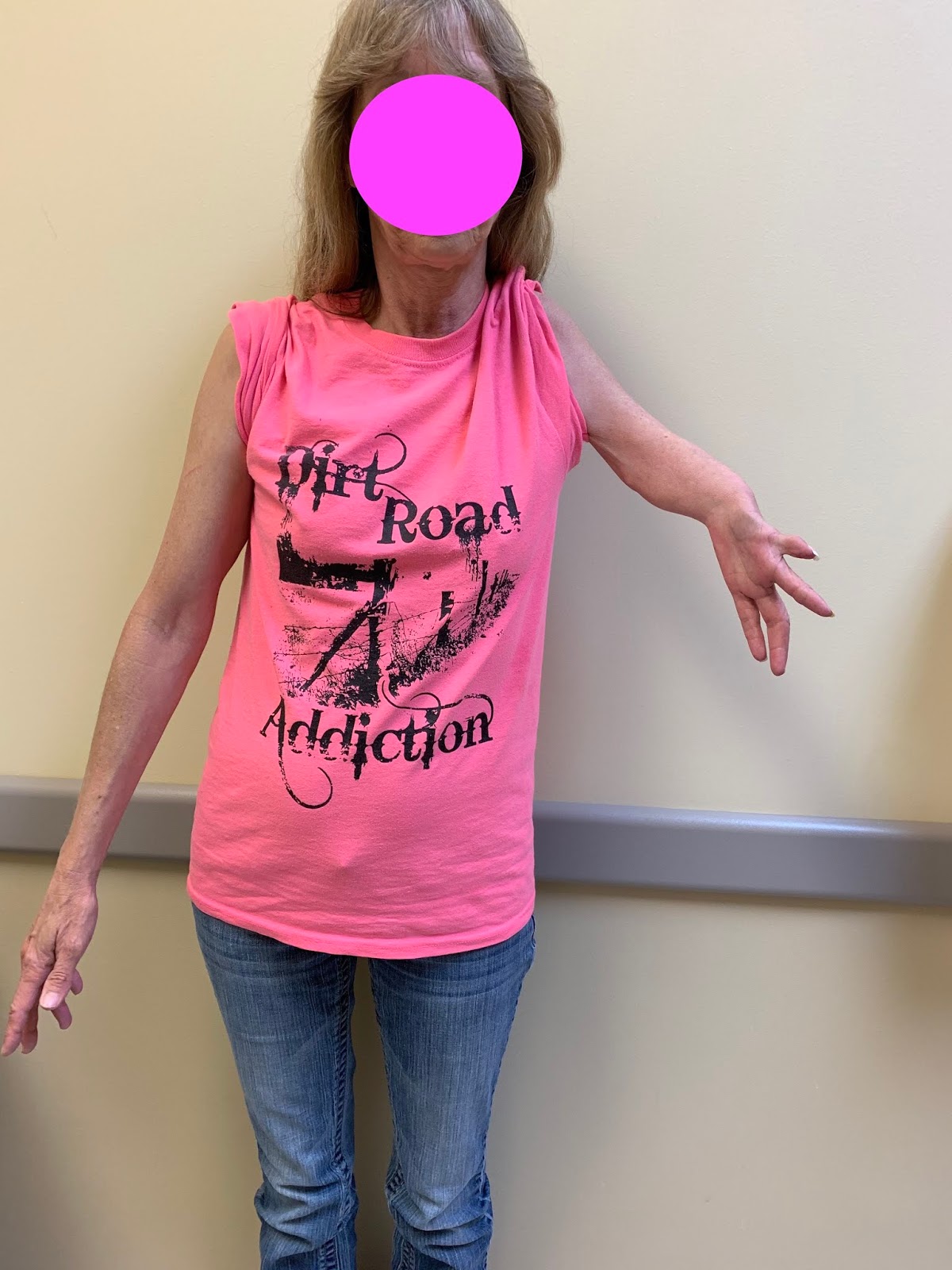
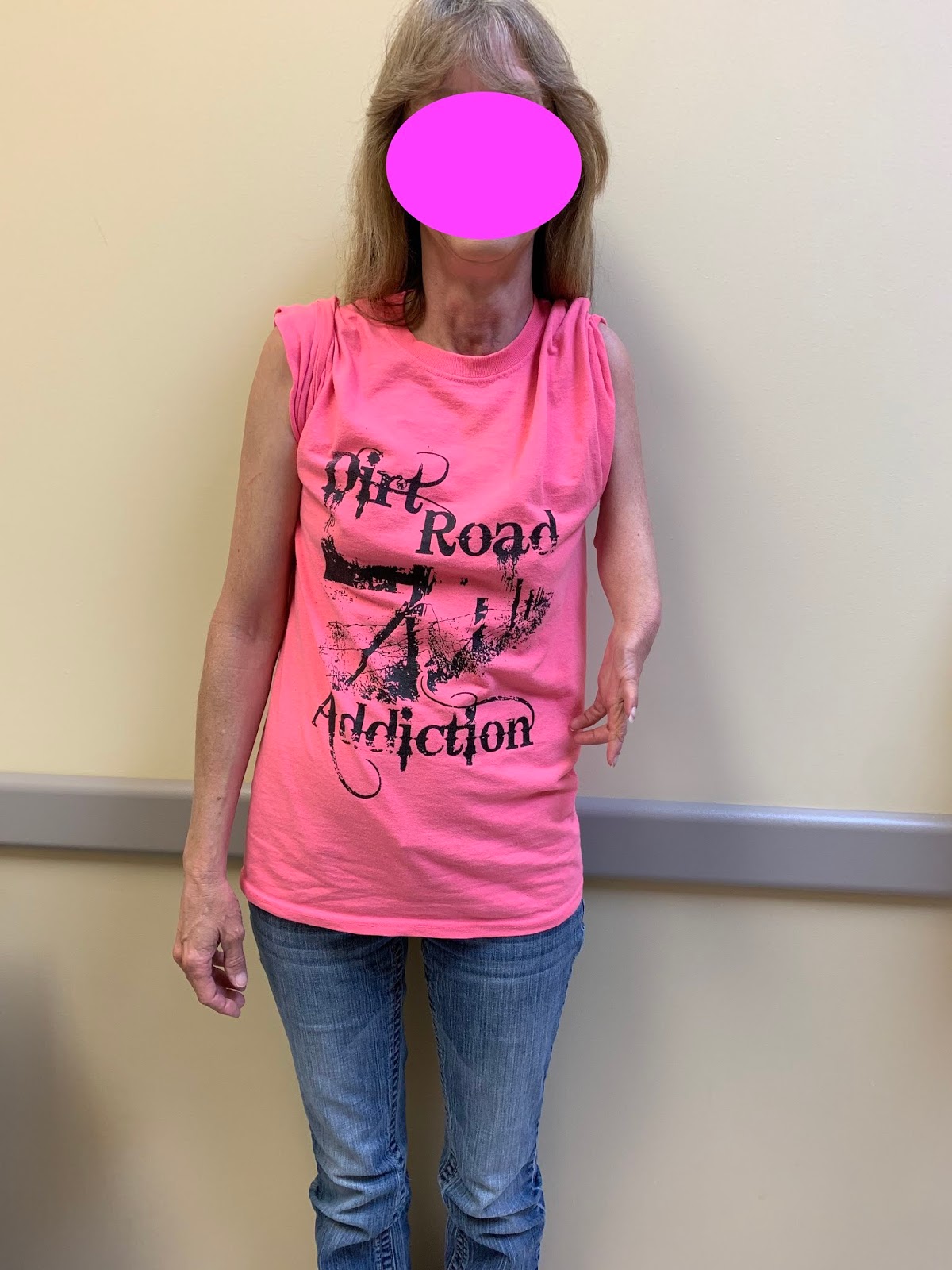
This patient had an isolated condition with a very short left upper extremity without elbow motion. Shoulder motion was also limited. Also, there was a thumb and three fingers with some limited motion of the fingers as well.
 |
| Appearance of ulnar deficiency. Note the very short arm, lack of elbow motion, and missing finger. |
 |
Appearance of ulnar deficiency. Note the very short arm, lack of elbow motion, and missing finger.
|
X-rays confirm the diagnosis of Type 5 ulnar longitudinal deficiency (also know as ulnar clubhand, ulnar hypoplasia, and ulnar amelia).
 |
| Type 5, severe, ulnar longitudinal deficiency. Not the abnormal shoulder, lack of elbow, and missing finger. |
 |
Type 5, severe, ulnar longitudinal deficiency. Not the abnormal shoulder, lack of elbow, and missing finger.
|