Amniotic constriction band is a common condition which typically involves more than one extremity. While the belly and face can be involved in rare patients, the arms and legs are the classic sites. Every child with amniotic band is different. Totally. Sometimes, physicians refer to it as a syndrome but that is not really accurate- it is a random pattern of constriction rings, amputations, and syndactylies (classically, what we call these fenestrated syndactyly- that is syndactyly with a hole between the fingers). Because every child is different, treatment is developed for each child. But treatment is also not always required, thankfully. This is the very brief story of one amazing child who has done well and is so happy with his new thumb.
The goal in the treatment of a hand with notable finger loss is to assure (when possible) that the child has at least two fingers (ideally a finger and a thumb) for pinch. This is, of course, even more important when both hands are involved and when one hand is completely absent.
This adopted patient presented with amniotic constriction band and a midforearm deficiency on the right and multiple finger amputations with a short thumb on the left.
 |
| Amniotic constriction band affecting both arms. There is no hand on the right and a limited hand, as seen better below, on the left. |
 |
| A child with amniotic constriction band before treatment. Not the normal little finger, short ring finger, very short pointer and middle finger and very short thumb. |
 |
| This x-ray confirms the amniotic constriction band diagnosis with a normal little finger, short ring finger, and very short thumb, pointer, and middle fingers (really only the hand bones- the metacarpals). |
The patient was struggling grasp and pinch. We met the family several times and elected to proceed with a lengthening procedure of the thumb metacarpal to improve pinch against the ring and small fingers. This requires at least two surgeries
– one surgery to ‘break’ the bone and apply the fixator
– a second to remove the fixator and deepen the first web space to ease the pinch motion
-importantly for both child and family- this lengthening is done by turning a dial 2-4x each day and is completely painless.
I really like this operation but there can be challenges. And I have learned from my partners Eric Gordon and Mark Miller (see their site) who lengthen and straighten larger bones.
Precautions
– The bone does not always unite and this process take a long time
– Careful weekly x-rays allow monitoring and adjustment of the ‘turn’ rate
– Regular follow up to assure no infection or to treat pin tract infections (unfortunately, these are common).

This patient eventually healed but there was some deformity in the bone and we straightened it (a third simple surgery). He and his family are very happy with his function. We will, obviously, continue to follow the patient over time. He will likely benefit from a second operation in a few years and maybe even a third as a teen. But, in a child like this with a challenging presentation of amniotic constriction band, the surgeries will make a clear functional difference.
 |
| Patient after lengthening for amniotic constriction band. Note the length of the new thumb. |
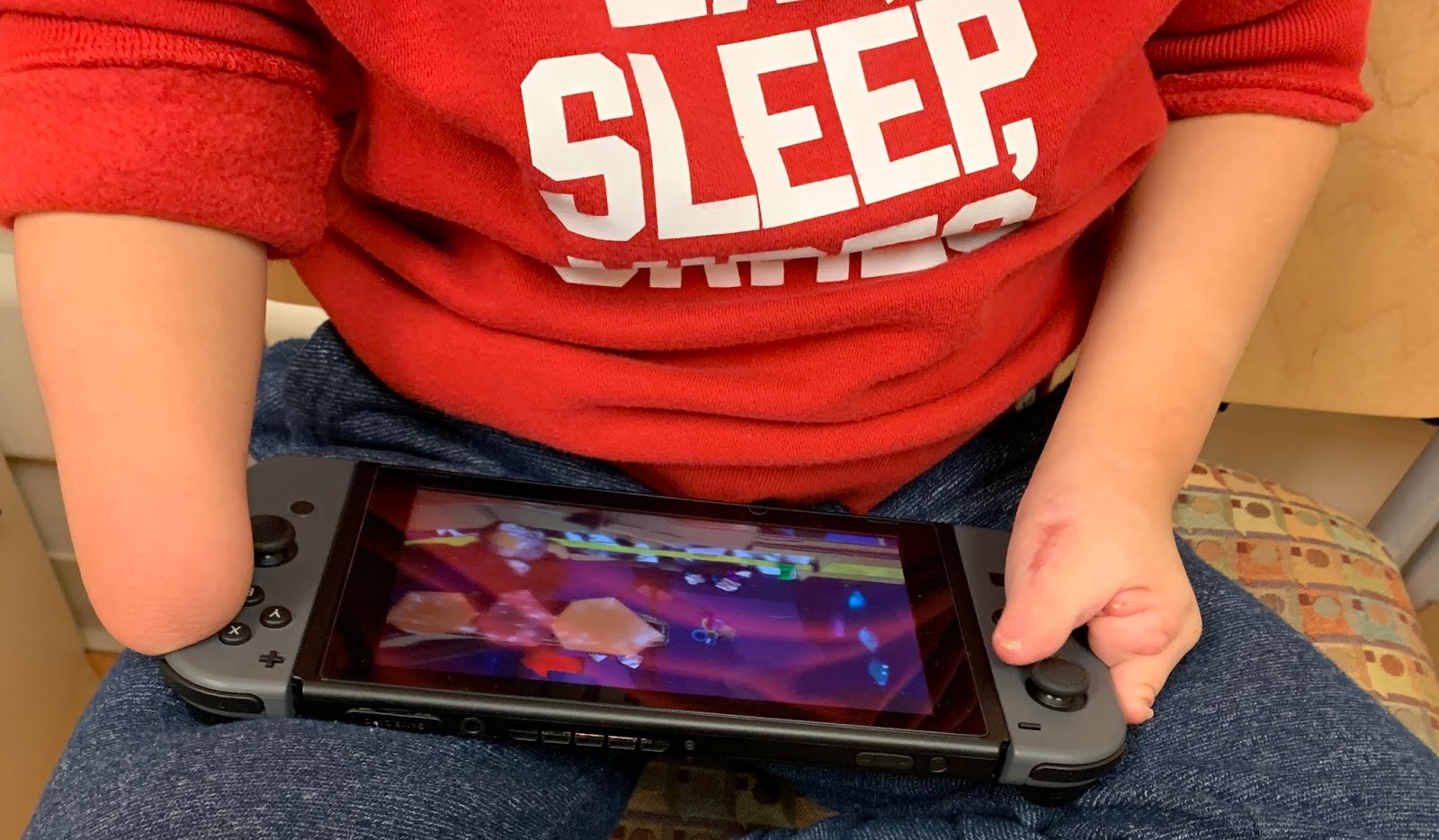 |
| Patient after lengthening for amniotic constriction band. Note the length of the new thumb. It is great to see him using the new thumb! |
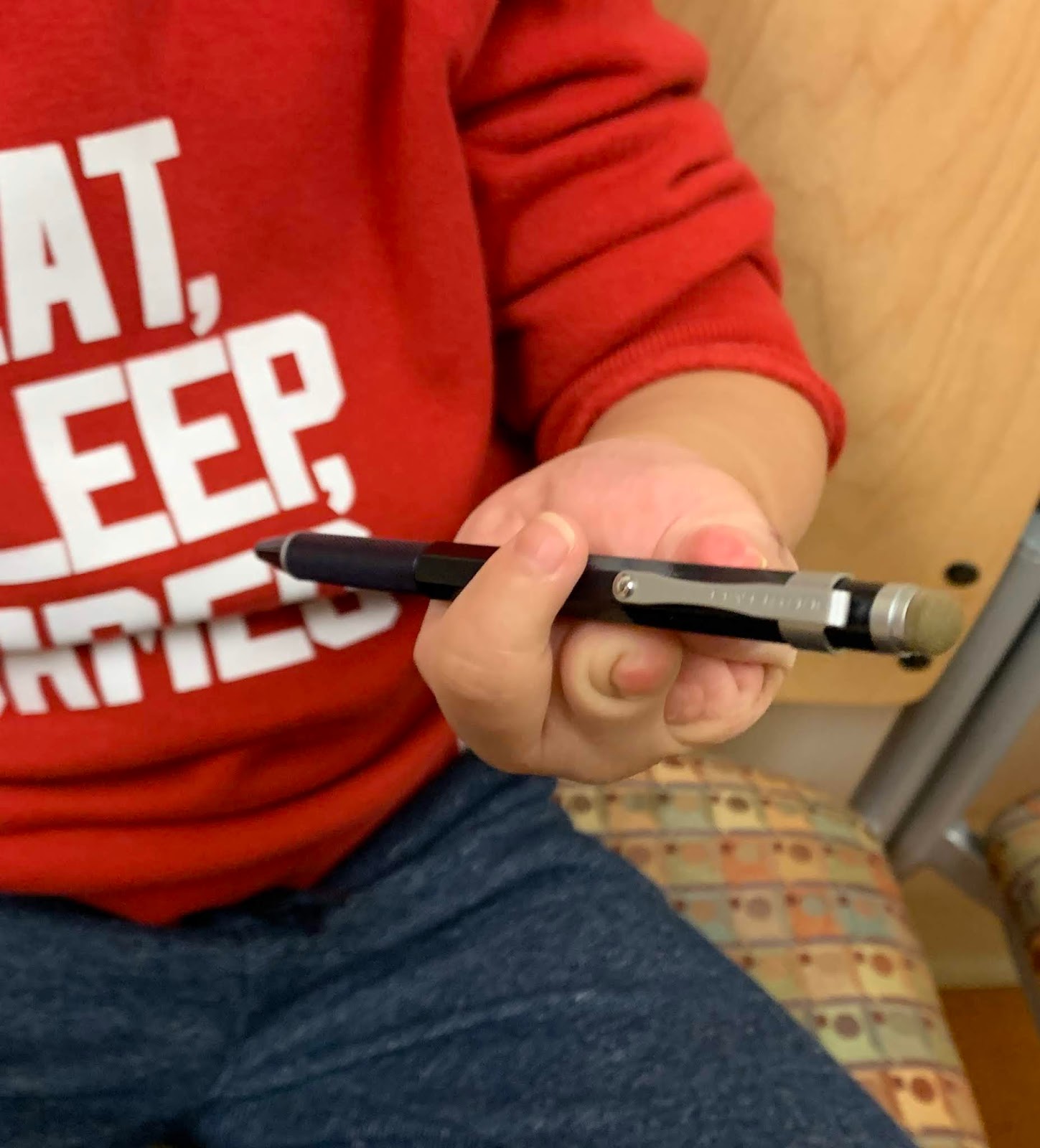 |
| Patient after lengthening for amniotic constriction band. Note the length of the new thumb. He uses the new thumb to write. |
 |
| Lengthened bone in amniotic constriction band. Not the length of the thumb metacarpal compared to the xray above. |
Charles A. Goldfarb, MD
email: congenitalhand@wustl.edu
Please CLICK HERE to support our research.
Designate my name. Thank you!