Birth differences of the upper extremity have many different forms/ presentations. These can be a dramatic with a shortened or deviated extremity or very subtle/ mild with slightly short fingers or a subtle lack of muscle development. In my three decades of caring for kids, it has always been clear that our team is truly caring for the whole family. Families have many questions about what we can do to help their child (surgery, therapy, what the future holds for their child, and the ‘why’- why is their chiild, their family affected with this anomaly. The purpose of this blog post is to discuss the last issue, the ‘why’ of birth differences of the upper extremity. This is part 1 and I will add a part 2 with some specific information about different anomalies. I always share with patients that limb differences are most commonly related to errors to our genetic code- the DNA. This means that there are changes (mutations) in the DNA sequences related to errors in the coding. We believe that some of these are random (just happen), some are clearly a genetic condition (passed from parent to child), and some are caused by external causes that lead to the mutation. This can be related to medication, environment, or other causes of DNA changes. To me, the fact that our bodies get it ‘right’ as often as they do is really remarkable. I stress that in the vast majority of patients, nothing a parent did caused the mutation in the DNA and nothing they could have done would have prevented this error. This is really, really important because all parents question their “role”. Known examples of medications or drugs causing a limb difference are really uncommon. The most striking and perhaps the most understood example of a medication leading to an extremity difference is the drug thalidomide which was given in the 1950s and early 1960s to help prevent nausea of pregnancy. Thalidomide caused dramatic “phocomelia” or limb shortening. I have blogged about this before on several occasions: This is a classic image from Smithsonian magazine.

Our understanding of birth differences continues to grow but it is safe to say that we all want to know more. The first step in understanding why birth differences happen is understanding what normal (or maybe I should say typical) limb development looks like. We know that upper limb development occurs from 26-54 days of gestation- with the upper limb fully formed before the end of the second month of pregnancy (although obviously quite small). There are three axes of development each with each being guided by different proteins, signals, and morphogens. The axes all development and progress simultaneously and NOT independently- there is a complex interaction between these areas. 1) The proximal distal axis 2) The anterior posterior axis (also known as the radial- ulnar axis and the pre-axial- post axial axis) 3) The dorsal- volar axis (top and bottom of the limb and fingers) One of my favorite articles on limb development was written more than 20 years ago and it discusses one of the key morphogens- sonic hedgehog. Robert Riddle and Clifford Tabin share insights which have stood the test of time including the importance of this video game inspired name of a key protein.

There have been many experiments to better understand limb development and some of my favorites use chick embryos. The developing limb can be easily altered to assess the impact of different proteins or areas of the developing limb. Cheryl Tickle has made notable contributions in this field as higlighted . Below I share a few images from my friend and limb development expert Kerby Oberg. Kerby has made so many contributions to the field is a close friend to clinicians who focus on the treatment of kids with limb differences. He is also a part of the team that created the very important and practical classification system for upper limb anomalies- the OMT. We recently updated the classification system as part of a great team.

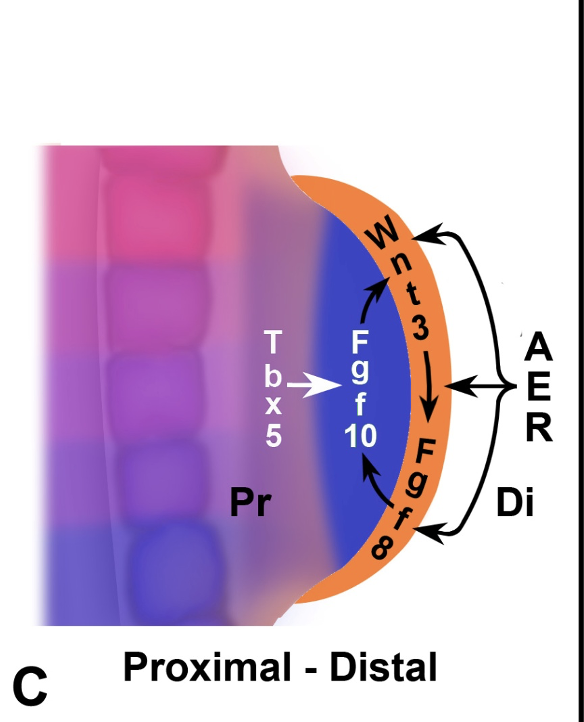
The proximal distal axis This axis of development is all about the limb growing longer and bigger. The apical ectodermal ridge (AER) is the key area of ectoderm that interacts with the underlying mesoderm to grow the limb. This limb is affected dramatically by TBX5, Wnt3, FGF8 and FGF10.
The anterior posterior axis This axis is guided by sonic hedgehog (as noted above). This protein diffuses across the developing limb and is key for ulnar sided limb development. Too little contributes to ulnar deficiency and extra (especially in a different area) can lead to a mirror hand. Radial deficiency is likely more related to Gli3 but this is a complicated interchange.

The dorsal ventral axis This axis is least well understood and, perhaps, least ‘important’ to limb development. Classically, we think about LMXb1 as driving the difference in function and appearance between the top and bottom of the fingers.

My next post will be more on what we know about specific conditions and what might go wrong during limb development. Thanks for reading, Charles A. Goldfarb, MD My Bio at Washington University email: congenitalhand@wustl.edu Please CLICK HERE to support our research. Designate my name. Thank you!
Looking forward to the second post in this series