It has been far too long since my post on the “Why” of Birth Differences. I apologize and I know at least some of you have been awaiting this post. No excuses but I am now on a new platform and the transition took time. This is Part 2 in which I will review some of the common birth differences and share what we know about these conditions. While I hope my post is helpful, there are a few other very good websites that dive into the specifics- some of these a bit more technical/ scientific. I have used these sites as resources to help relay the current understanding of these conditions (at a non- geneticist level). A few of my favorite sites:
This post is meant to be used in combination with Part 1 which includes information on upper extremity development. There are many, many upper extremity birth conditions but I briefly discuss the genetics behind a few of these. Our CoULD Registry is a good reference point point- here are its top 5 conditions:
- Radial polydactyly
- Small thumb (hypoplastic thumb)
- Ulnar polydactyly
- Symbrachydactyly
- Syndactyly
Lets begin with a basic review of genetics. In 2011, the Human Genome Project was completed and it gave us unbelievable information. There are 3 billion base pairs and humans are remarkably similar- about 99% of our DNA is the same no matter our race, sex, etc. Most of the human genome is the intron (97%) – that is the space between the key coding areas called exons (only 3% of our DNA and only 78 million base pairs). More to come on all of this with an upcoming post- genetic testing (Part 3). To simplify, if genetics are involved in the development of an upper extremity birth difference, there is an error in the coding or reading of the exons but we continue to learn more every day about this process. Processes in the area of the intron also can affect our unique DNA and can also, we believe, lead to upper extremity anomalies.
Common Conditions
Ulnar Longitudinal Deficiency
The ulnar side means the pinky side of the hand and forearm. This deficiency can affect the whole limb and has been shown to be related to an area of development in the limb bud called the zone of polarizing activity (ZPA) on the posterior part of the limb bud. That is the site of origin of a protein called sonic hedgehog (Shh). This protein (its actually called a morphogen) diffuses across the developing limb bud and it vital for the development of the ulnar sided structures. So, without Shh, we see Ulnar Longitudinal Deficiency (ULD) of some kind. We know that timing is everything- the earlier the insult, the more severe the difference. There may be a specific genetic issue leading to ULD but these are often unilateral and some believe that a physical or chemical insult to the ZPA may be responsible for some. The genetics are less well understood with ulnar mammary syndrome being one of the few presentations with well understood genetics related to the TBX3 gene. We classify ULD from Type 0 (hand affected only) to Type 5 (entire limb is shortened, no elbow motion). Many of the kids from my previous post with “phocomelia” in reality likely have ULD- just the most severe type.

Radial Longitudinal Deficiency (RLD)
I started with ULD because it seems more straightforward (even though I left out some of the deeper details). RLD is much more common than ULD. The reasons for that are likely many but include the fact that the insults related to ULD happen earlier and are more likely fatal to the developing fetus (we know this from interesting rat studies from Japan). RLD is also far more likely to be associated with a syndrome which I will briefly highlight below. But just like there is an “ulnarizing” effect of the Shh, there is a radializing effect of the molecule Gli3r. The fingers are super interesting and complex in their development. Development of the thumb is separate from the fingers and is associated with Gli3- which is why kids with RLD typically also commonly have a thumb development issue. Milder RLD may only demonstrate a small thumb.
VACTERL Association. This is an association of findings (vertebral, anal atresia, trachea esophageal fistula, cardiac, renal) and is typical a sporadic finding without known genetic underpinnings.
Holt Oram Syndrome. This is autosomal dominant meaning one affected parent has a 50% chance of passing it to each child. If the child has the gene, he or she will have Holt Oram Syndrome. We believe that a mutation in the TBX5 gene causes this condition.
TAR syndrome. Thrombocytopenia absent radius. This is autosomal recessive which means that both parents must have the gene and only when each parent passes the gene to the child will we see it (so 25% of their children will have TAR Syndrome). Mutations in the RBM8A gene cause TAR syndrome.
Fanconi Anemia. This is most often autosomal recessive (can be sex linked recessive) and is caused by a mutation in the FANC genes . Upper extremity presentation can vary and patients are typically short stature and may have cafe au lait spots. This condition is unique amongst other causes of radial deficiency as it may be fatal. Early genetic testing can identify this genetic abnormality and allow treatment.

Madelung Deformity
Madelungs is thought to be related to limited development of a portion of the growth plate of the distal radius but I believe it is more complex than this. While there can be isolated Madelungs, it can also be associated with a syndrome: short stature, short forearms, and Madelungs- Léri-Weill dyschondrosteosis. We know that the SHOX gene is mutated in children with this condition. A more severe form with absence of both SHOX genes is called Langer mesomelic dysplasia.

Extra pinky finger (aka post axial polydactyly)
There are a few clear facts about this condition. First, it is most common in African Americans (10:1 vs Caucasian) and is dramatically more common than all other types of extra fingers. It is most often passed down as autosomal dominant (an affected parent has a 50% chance of passing it to each child). Some evidence points to Gli3 but the explanations are likely multiple.
Extra Thumb (aka, preaxial polydactyly).
Thumb polydactyly is less clear in its origin, less clear in its genetics, and far less common compared to extra pinkies. There have been multiple pathways identified with multiple genes identified and different inheritance patterns. We do believe Gli3 is often the issue.

Cleft Hand
Cleft hand may be isolated and affect only one hand or may be part of a condition called split hand foot malformation. There is a huge amount of genetic information with numerous explanations for split hand foot malformation including autosomal dominant and recessive inheritance.

Syndactyly
In my experience, most children with syndactyly have no known genetic risk factors or affected family members. However, there are numerous genes which have been implicated and some families do have dominant or recessive inheritance. One syndrome is ODDD- oculodental digital dysplasia which includes syndactyly and is autosomal recessive, affecting the GJA1 gene.

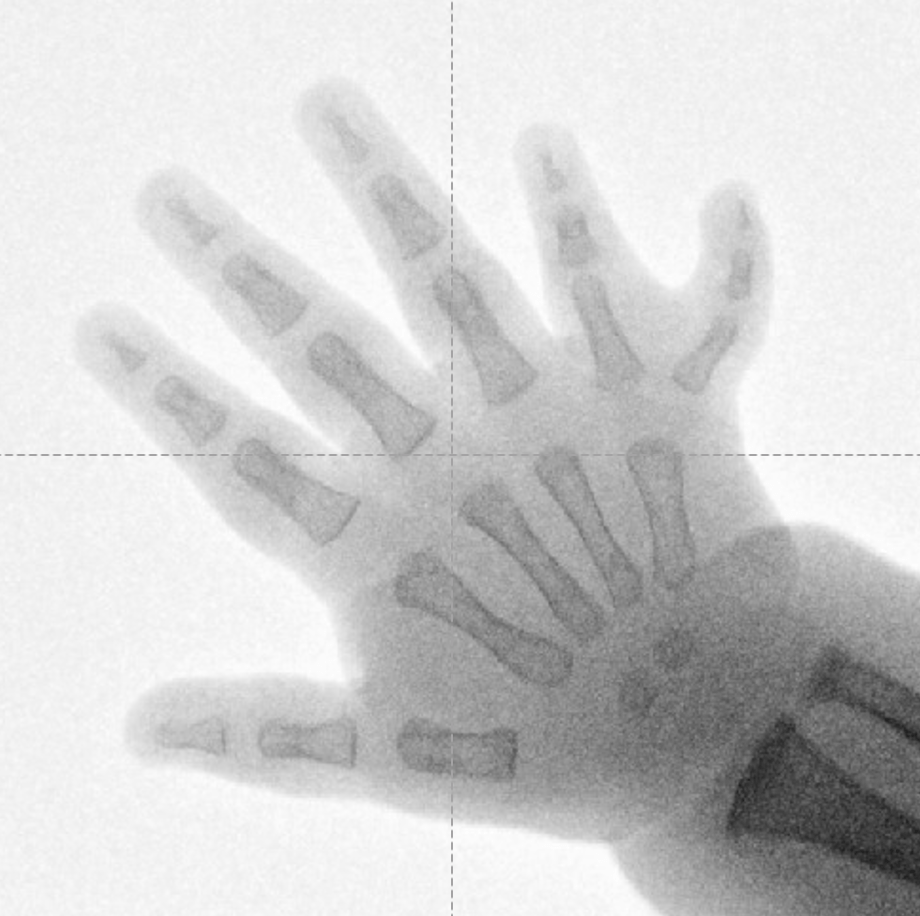
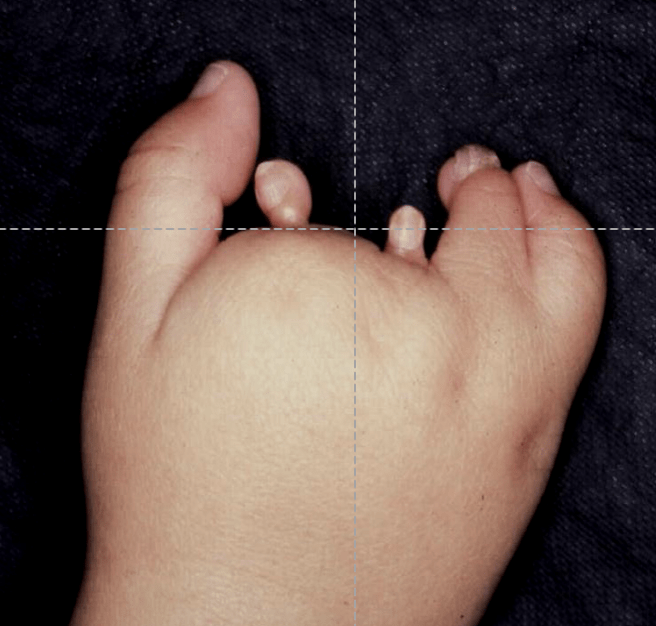
Symbrachydactyly
This condition is considered non- syndromic and non genetic. We believe it is related to an insult to the blood supply of the developing limb. However, patients present in relatively typical ways- for example, when the forearm is affected, the limb development seems to always stop in the proximal 1/3rd of the forearm. Perhaps this suggests that there is a more specific insult or a genetic cause for this condition as well.
Summary
I hope this information is helpful. As noted, please use this together with the information in Part I. Shortly, I will add a Part III which will discuss genetic testing and how we think of it in our field. Finally, remember that this is an exciting time for this field as our understanding of limb development and genetic anomalies continues to improve. Thanks as always to Kerby Oberg who has taught me so much about limb development and birth differences in general.